Abnormal Fetal Position and Presentation
Under normal circumstances, a baby is in the vertex (cephalic) position before delivery. In the vertex position, the baby’s head is at the lower part of the abdomen, and the baby is born head-first. However, some babies present differently before delivery. Abnormal presentations may place the baby at risk of experiencing umbilical cord problems and/or a birth trauma.
What is the difference between fetal presentation and position?
In the womb, a fetus has both a presentation and a position.
- Presentation refers to the part of the baby’s body that leads out of the birth canal. For example, if a baby’s rear is set to come out of the birth canal first, the baby is said to be in “breech presentation.”
- Position refers to the direction the baby is facing in relation to the mother’s spine. A baby could be lying face-first against a mother’s spine or face up towards the mother’s belly.
What way should a baby come out during birth?
Vertex presentation is the ‘normal’ position for birth and the lowest-risk presentation for vaginal birth.
In vertex presentation, the baby is positioned head-first with back of the head entering the birth canal first. In this position, the baby’s chin is tucked into their chest and they are facing the mother’s back (occipito-anterior position).
Any position other than vertex position is abnormal and can make vaginal delivery much more difficult or sometimes impossible. If a baby’s chin isn’t tucked into their chest, they may come out face-first (face presentation), which can cause birth injury.

What happens if a baby isn’t in the standard vertex position during birth?
Before vaginal delivery, the baby must be in the standard vertex presentation and within the normal range for weight and size. This helps ensure the safety of both baby and mother during labor.
When the baby’s size or position is abnormal, physicians should usually intervene. This may mean simple manual procedures to help reposition the baby or, in many cases, a planned C-section delivery. Healthcare professionals must identify and quickly resolve issues related to fetal size, weight, and presentation. Failing to intervene is medical malpractice.
Numerous complications may result from abnormal weight, size, abnormal position, or abnormal presentation.
Should I contact a lawyer?
Abnormal presentation, if mishandled, can cause birth injuries. If you have any concerns about your baby’s labor and delivery, a consultation with an attorney is completely free. A birth injury lawyer can provide insight about potential medical malpractice.
Compound presentation
In a compound presentation, there are multiple presenting parts. Most commonly, the baby’s head and an arm come out at the same time. Sometimes compound presentation can occur with twins where the head of the first twin presents with the extremity of the second twin.
Risk factors for compound presentation include:
- Prematurity
- Intrauterine growth restriction (IUGR)
- Multiple gestations (twins, triplets, etc.)
- Polyhydramnios (too much amniotic fluid)
- A large pelvis
- External cephalic version
- Rupture of membranes at high station
Compound presentations can be detected via ultrasound before the mother’s water breaks. During labor, a cervical examination finds compound presentation.
If a mother has polyhydramnios, the risk of compound presentation is higher. The flow of amniotic fluid when the membranes rupture can sweep extremities into the birth canal or cause a cord prolapse, which is a medical emergency.
If compound presentation continues, it is likely to cause dystocia (the baby becoming stuck in the birth canal), which is also a medical emergency. Often, the safest way to deliver a baby with compound presentation is C-section.
Complications like dystocia and cord prolapse carry risks of severe adverse outcomes, including cerebral palsy, intellectual and developmental disabilities, and hypoxic-ischemic encephalopathy (HIE).
Limb presentation
Limb presentation during childbirth means that the part of the baby’s body that emerges first is a limb – an arm or a leg. Babies with limb presentation cannot be delivered safely via vaginal delivery. They must be delivered quickly by emergency C-section.
Limb presentation poses a large risk for dystocia, which is a medical emergency.
Occipitoposterior (OP) position
In occipitoposterior (OP) position, the baby is head-first with the back of the head turned towards the mother’s back. This position is also called an occiput posterior position. The baby’s head can be rotated to the right (right occipitoposterior position, or ROP), or to the left (left occipitoposterior position, or LOP).
Approximately 1 out of 19 babies present in a posterior position rather than an anterior position.
Occipitoposterior position increases the baby’s risk of experiencing:
- prolonged labor
- prolapsed umbilical cord
- forceps and vacuum extractor injuries
- brain bleeds
- a lack of oxygen to the brain
- Hypoxic-ischemic Encephalopathy (HIE)
If a manual rotation cannot be quickly and effectively performed in the face of fetal distress, the baby should be delivered via C-section. A C-section can help prevent oxygen deprivation caused by complications with OP position.
A nurse explains posterior position
Breech presentation
Breech presentation is normal throughout pregnancy. However, by the 37th week, the baby should change positions in time for labor. Breech presentation occurs when a baby’s buttocks or legs are positioned to descend the birth canal first. Breech positions are dangerous. During a vaginal delivery, a baby is at increased risk for serious problems with labor.
Most experts recommend C-section delivery for all types of breech positions because it is the safest method of delivery and it helps avoid birth injuries (6). Mismanaged breech birth can result in the following conditions:
- Traumatic birth
- brain bleeds (intracranial hemorrhages)
- Spinal cord fractures
- Hypoxic-ischemic encephalopathy (HIE)
- Seizures
- Cerebral palsy
- Intellectual disabilities
- Developmental delays
Dealing with a birth injury can be difficult, but our attorneys can help.
Face presentation
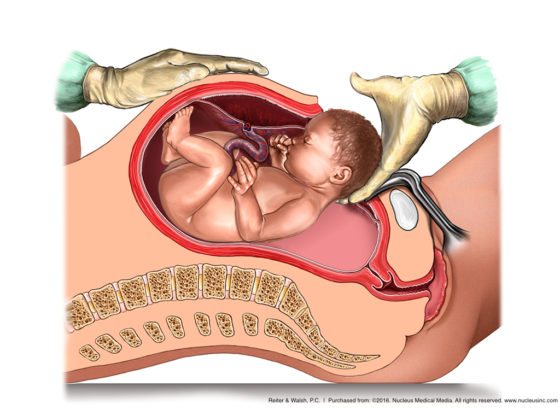
A baby usually tucks its chin so they can be born head-first. A face presentation occurs when the face is the presenting part of the baby. In this position, the baby’s neck is extended backward. The back of the head touches the baby’s back. This prevents head engagement and descent of the baby through the birth canal.
In some cases of face presentation, the trauma of a vaginal delivery causes face deformation and fluid build-up (edema) in the face and upper airway. The baby will often need a breathing tube placed in the airway to maintain airway patency and assist breathing.
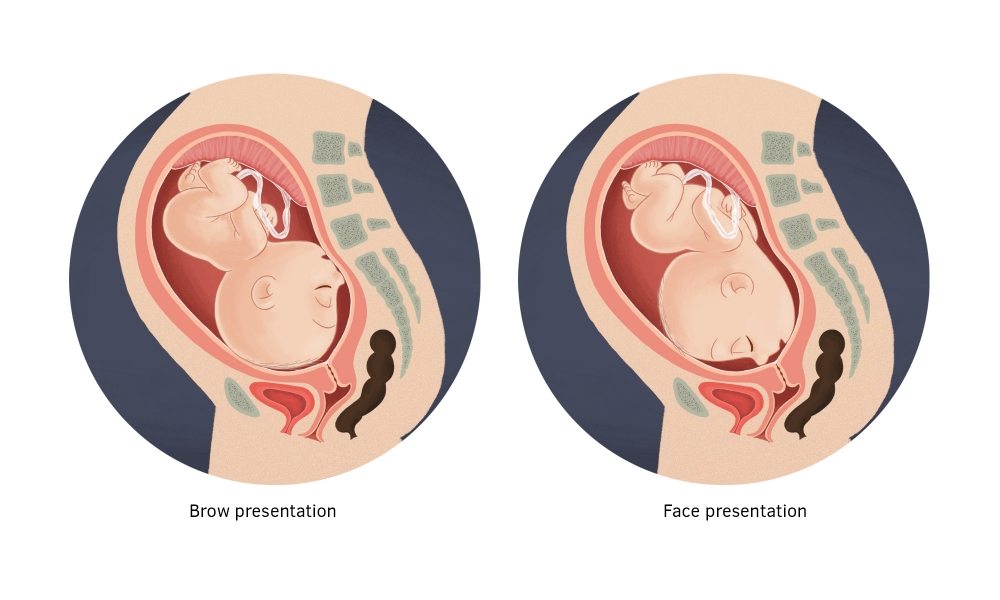
Image by healthhand.com
Trauma is very common during vaginal delivery of a baby in face presentation. Medical staff must warn parents that their baby may be bruised and that a C-section is available to avoid this trauma.
When face presentation occurs, experts recommend liberal use of C-section.
Complications of Mismanaged Face Presentation
- Prolonged labor
- Facial trauma
- Facial and upper airway edema (fluid build-up in the face, often caused by trauma)
- Skull molding (abnormal head shape that results from pressure on the baby’s head during childbirth)
- Respiratory distress or difficulty in ventilation (the baby being able to move air in and out of lungs) due to upper airway trauma and edema
- Spinal cord injury
- Abnormal fetal heart rate patterns
- 10-fold increase in fetal compromise
- Brain bleeds
- Intracranial hemorrhages
- Hypoxic-ischemic encephalopathy (HIE)
- Permanent brain damage
- Cerebral palsy
- Seizures
- Intellectual disabilities
- Developmental delays
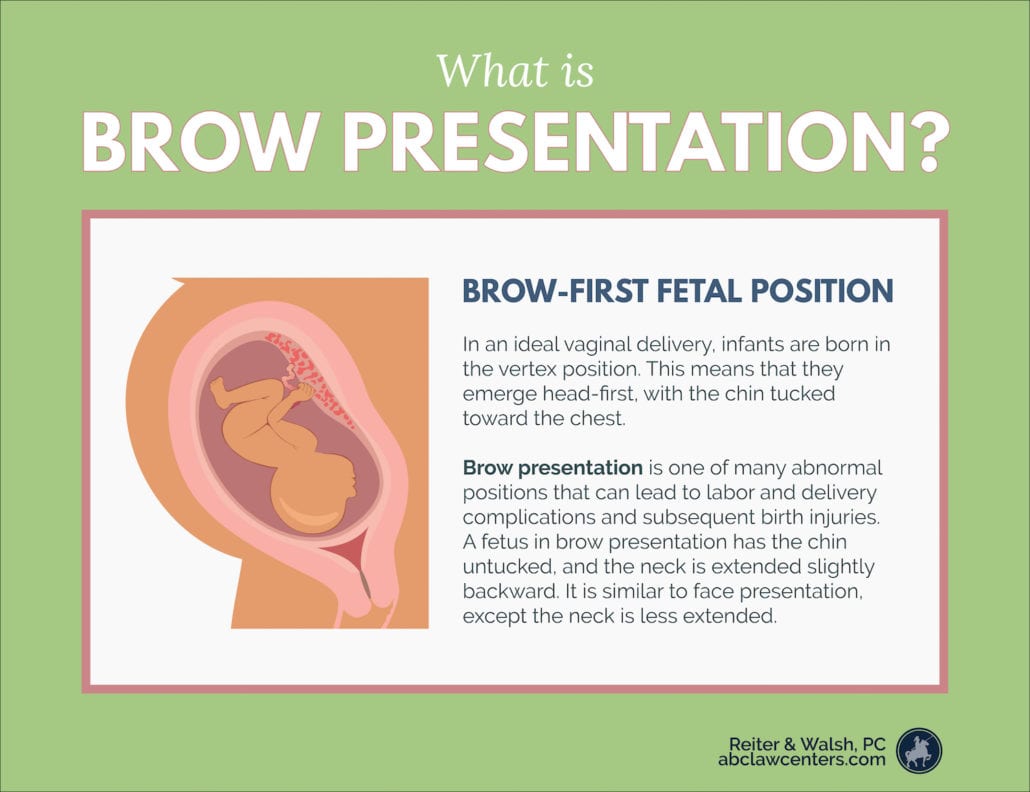
Brow presentation
Brow presentation is similar to face presentation, but the baby’s neck is less extended. A fetus in brow presentation has the chin untucked, and the neck is extended slightly backward. The brow (forehead) is the part situated to go through the pelvis first. Vaginal delivery can be difficult or impossible with brow presentation, because the diameter of the presenting part of the head may be too big to safely fit through the pelvis.
Risk factors and conditions associated with brow presentation
Brow presentation has been linked to several risk factors and co-occurring conditions. These include:
- Multiparity (having previously given birth)
- Premature delivery
- Fetal anomalies, such as
- anencephaly (an absence of major parts of the brain and skull)
- anterior neck mass (a growth on the front of the neck)
- Previous c-section delivery
- Polyhydramnios (excessive amniotic fluid)
Diagnosis of brow presentation
Brow presentation can often be diagnosed through a vaginal examination during labor. If there are no conclusive signs from the physical examination, an ultrasound can show brow presentation.
Warning signs of brow presentation may include signs of fetal distress or lack of labor progression.
Management of brow presentation
Infants in brow presentation early in labor may spontaneously move into a safer position during the delivery process. Safe delivery in brow presentation may be possible if the infant is small and/or the mother’s pelvic opening is large. For these reasons, physicians occasionally recommend vaginal delivery of infants in brow presentation.
Doctors attempting vaginal delivery of a baby in brow presentation must watch for signs of fetal distress, such as an abnormal heart rate. Signs of fetal distress can indicate that a baby is in danger of sustaining serious brain injury. Quick intervention can prevent harm to the baby.
Medical staff should also monitor progression of labor when attempting a vaginal delivery of a baby in brow presentation. Prolonged labor can cause extended periods of fetal oxygen deprivation, which can cause birth asphyxia and permanent injury.
If an infant in brow presentation begins to show signs of distress, or if labor progress stops or slows significantly, physicians should be ready to move on to a cesarean delivery.
Labor induction or augmentation with the drug Pitocin (synthetic oxytocin) is very dangerous in cases of brow presentation. Pitocin can lead to excessive uterine contractions. The contractions can put pressure on the infant’s head and cut off their oxygen supply. In cases of brow presentation, usage of Pitocin is risky when the baby is not positioned for safe delivery.
Complications of brow presentation
Physicians can diagnose brow presentation early. When appropriately managed, delivery
can typically occur with no serious negative effects on the mother or baby.
However, if medical professionals fail to recognize brow presentation and intervene as necessary, there can be lasting consequences. Infants may suffer oxygen deprivation due to prolonged labor, or traumatic injuries from a difficult delivery. Some of the most severe conditions resulting from mismanaged brow presentation births include:
Shoulder presentation (transverse lie)
Shoulder presentation (transverse lie) is when the arm, shoulder or trunk of the baby enter the birth canal first. When a baby is in a transverse lie position during labor, C-section is almost always used as the delivery method.
These situations make transverse lie position more likely:
- polyhydramnios (too much amniotic fluid)
- Multiples pregancy
- placenta previa
- a baby with intrauterine growth restriction (IUGR)
Once the membranes rupture, there is an increased risk of umbilical cord prolapse in this position. A C-section should ideally be performed before the membranes break. Failure to quickly deliver the baby by C-section when transverse lie presentation is present can cause severe birth asphyxia due to cord compression and trauma to the baby. This can cause hypoxic-ischemic encephalopathy (HIE), seizures, permanent brain damage, and cerebral palsy.


Legal help for birth injuries from abnormal position or presentation
The award-winning birth injury attorneys at ABC Law Centers: Birth Injury Lawyers have over 100 years of joint experience handling birth trauma cases related to abnormal position or presentation. If you believe your loved one’s birth injury resulted from an instance of medical malpractice, you may be entitled to compensation from a medical malpractice or personal injury case. During your free legal consultation, our birth injury attorneys will discuss your case with you, determine if negligence caused your loved one’s injuries, identify the negligent party, and discuss your legal options with you.



Featured Videos
Posterior Position
Hypoxic-Ischemic Encephalopathy (HIE)

Featured Testimonial
What Our
Clients Say…
After the traumatic birth of my son, I was left confused, afraid, and seeking answers. We needed someone we could trust and depend on. ABC Law Centers: Birth Injury Lawyers was just that.
- Michael
Helpful resources
- Julien, S., and Galerneau, F. (2017). Face and brow presentations in labor. Retrieved from https://www.uptodate.com/contents/face-and-brow-presentations-in-labor.
- World Health Organization, UNICEF, and United Nations Population Fund. Malpositions and malpresentations. Retrieved from http://hetv.org/resources/reproductive-health/impac/Symptoms/Malpositions__malpresetations_S69_S81.html.
- Barth, W. (2016). Compound fetal presentation. Retrieved from https://www.uptodate.com/contents/compound-fetal-presentation.
- Gabbe, S.G., … Grobman, W.A. (2017). Compound Presentation. Retrieved from https://expertconsult.inkling.com/read/gabbe-obstetrics-normal-problem-pregnancies-7e/chapter-17/compound-presentation.
- Argani, C.H. and Satin, A.J. (2018) Occiput posterior position. Retrieved from https://www.uptodate.com/contents/occiput-posterior-position.
- Hofmeyr, G.J. (2018). Overview of issues related to breech presentation. Retrieved from https://www.uptodate.com/contents/overview-of-issues-related-to-breech-presentation.
- Hofmeyr, G.J. (2017). Delivery of the fetus in breech presentation. Retrieved from https://www.uptodate.com/contents/delivery-of-the-fetus-in-breech-presentation.
- Strauss, R.A. (2017). Transverse fetal lie. Retrieved from https://www.uptodate.com/contents/transverse-fetal-lie.
- Moldenhauer, J.S. (2018). Abnormal Position and Presentation of the Fetus. Retrieved from https://www.merckmanuals.com/home/women-s-health-issues/complications-of-labor-and-delivery/abnormal-position-and-presentation-of-the-fetus.