Premature Birth and Its Prevention
If a baby is born before 37 weeks of gestation, they are considered premature. Premature babies (also called “preemies”) are at a higher risk of medical issues because their organs are underdeveloped and easily damaged by birth injuries or complications in early infancy (1).
Every year, 15 million babies are born preterm (2). Premature birth is often preventable – doctors can prolong a pregnancy to the proper time using the hormone progesterone or a procedure called cervical cerclage if they promptly diagnose issues that are risk factors for premature birth. Once these factors are diagnosed, physicians must tailor a customized health plan to help maintain the pregnancy and protect the health of both mother and baby. This plan varies greatly from case to case, given the wide variety of factors that can cause premature birth.
Complications of premature birth
When a baby is born preterm, they are not yet fully developed, which can predispose them to injuries (3). Some of the complications of premature birth include:
Under-developed lungs
Babies born preterm face complications involving the lungs because their lungs are one of the last things to develop in the womb (5). A doctor can check the maturity of the lungs while the baby is in the womb with a process called amniocentesis (6). This is when amniotic fluid is removed from the uterus for testing. In certain cases, a steroid injection of betamethasone can be given to the mother of a premature baby to speed up the maturity of their lungs.
Often the lungs of preemies cannot produce enough surfactant on their own yet, and surfactant is one of the key chemical compounds that help the lungs function and stay flexible and pliant (3). Without surfactant, the lungs stay stiff, which means they cannot expand and contract well enough to get the air they need. Because of this, preterm babies often need extra help breathing. Medical practitioners can provide surfactant to keep the lungs flexible. They can also help the baby’s breathing with methods like positive-pressure ventilation, or in some cases where both the baby’s heart and lungs need support, with extracorporeal membrane oxygenation (ECMO).
Other possible complications of premature birth include (3,4):
- Heart Problems: Premature babies commonly experience heart problems such as hypotension (low blood pressure) and patent ductus arteriosus (PDA).
- Temperature control problems: Premature babies don’t have the stored body fat of full-term infants and often can’t generate enough heat to restore what is lost. They can develop hypothermia.
- Brain problems: Premature babies are at greater risk of intraventricular hemorrhage and a variety of other brain injuries.
- Immune system problems: Premature babies have an underdeveloped immune system, which puts them at a higher risk of infection.
- Blood issues: Premature babies are at a higher risk of jaundice, anemia, and other blood issues.
- Metabolism issues: Premature babies often develop metabolism issues like hypoglycemia (low blood sugar).
- Gastrointestinal issues: The immature gastrointestinal systems of premature babies puts them at risk of many issues involving feeding.
Additionally, there are long-term conditions that are associated with premature birth. For more details, see our section “What kinds of conditions are associated with preterm birth?”
Breathing support: risk of overventilation and hypocarbia
One problem that can occur in babies born preterm is brain injury stemming from overventilation and hypocarbia. The human body’s regulatory mechanisms operate under specific ratios of CO2 and oxygen in the blood.
If a baby is ventilated at too high a setting, the amount of CO2 in their blood can drop below a safe level. This is known as hypocarbia. If hypocarbia continues for too long, this can cause brain injuries like periventricular leukomalacia (PVL), among others.
If a baby is over-ventilated, the pressure from the machine can also cause lung damage like bronchopulmonary dysplasia (BPD) and pneumothorax (when the baby’s lung collapses). This can cause long-term scarring in the lungs and can compromise how well oxygen is delivered to the baby’s brain and other organs.
Why is preventing preterm birth so important?
With proper support, babies delivered at 28 weeks or later usually do very well, and develop without long-term problems. Each additional week of gestation and 100-gram increase in birth weight (in the lower-to-mid ranges of gestational age and birth weight) greatly reduces mortality risk. The longer a baby gestates, the less likely it is they will have a prematurity-related injury (7).
There are ways that medical practitioners can decrease the risk of preterm birth, especially when analyzing a mother’s prior health history closely.
What kinds of conditions are associated with preterm birth?
Possible long-term complications of premature birth include (5):
- Cerebral palsy: Premature babies are more susceptible the brain injuries, infection, and blood flow issues that bring about cerebral palsy, a movement disorder that affects muscle tone, movement, balance, and coordination.
- Hypoxic-ischemic encephalopathy (HIE): Some of the short-term complications of premature birth can lead to HIE, a neonatal brain injury caused by oxygen deprivation and/or limited blood flow to the brain at or near the time of birth.
- Developmental disabilities: Some of the short-term complications of premature birth can lead to developmental disabilities including cognitive and behavioral issues.
Preventing preterm birth
First and foremost, it’s very important for medical practitioners to take a full and accurate health history of the mother to identify any potential risk factors for preterm birth. If a mother has these risk factors, doctors and nurses should monitor her pregnancy more closely than that of a mother without risk factors. This will often mean more appointments with different kinds of assessments – the exact details vary from mother to mother.
What kinds of factors could contribute to preterm birth?
Some of the risk factors for preterm birth include (3):
- Prior history of preterm birth (increases the risk of premature birth by 10-35%)
- Prior history of short/insufficient cervix (25mm or less) (increases the risk of premature birth by 30-60%)
- Evidence of debris or sludge on ultrasound
- Maternal age (under 16 or over 25)
- Low socioeconomic status
- Presence of:
- Infection (chorioamnionitis or bacterial vaginosis)
- Hypertension
- Preeclampsia
- Diabetes
- Cardiovascular disorders
- Polyhydramnios (excessive amniotic fluid levels)
- Multiple gestations (twins, triplets, and other multiples)
- Placenta previa
- Placental abruption
- Interval of less than six months between pregnancies
Depending on a mother’s health history, the kinds of interventions that may be recommended can differ (3):
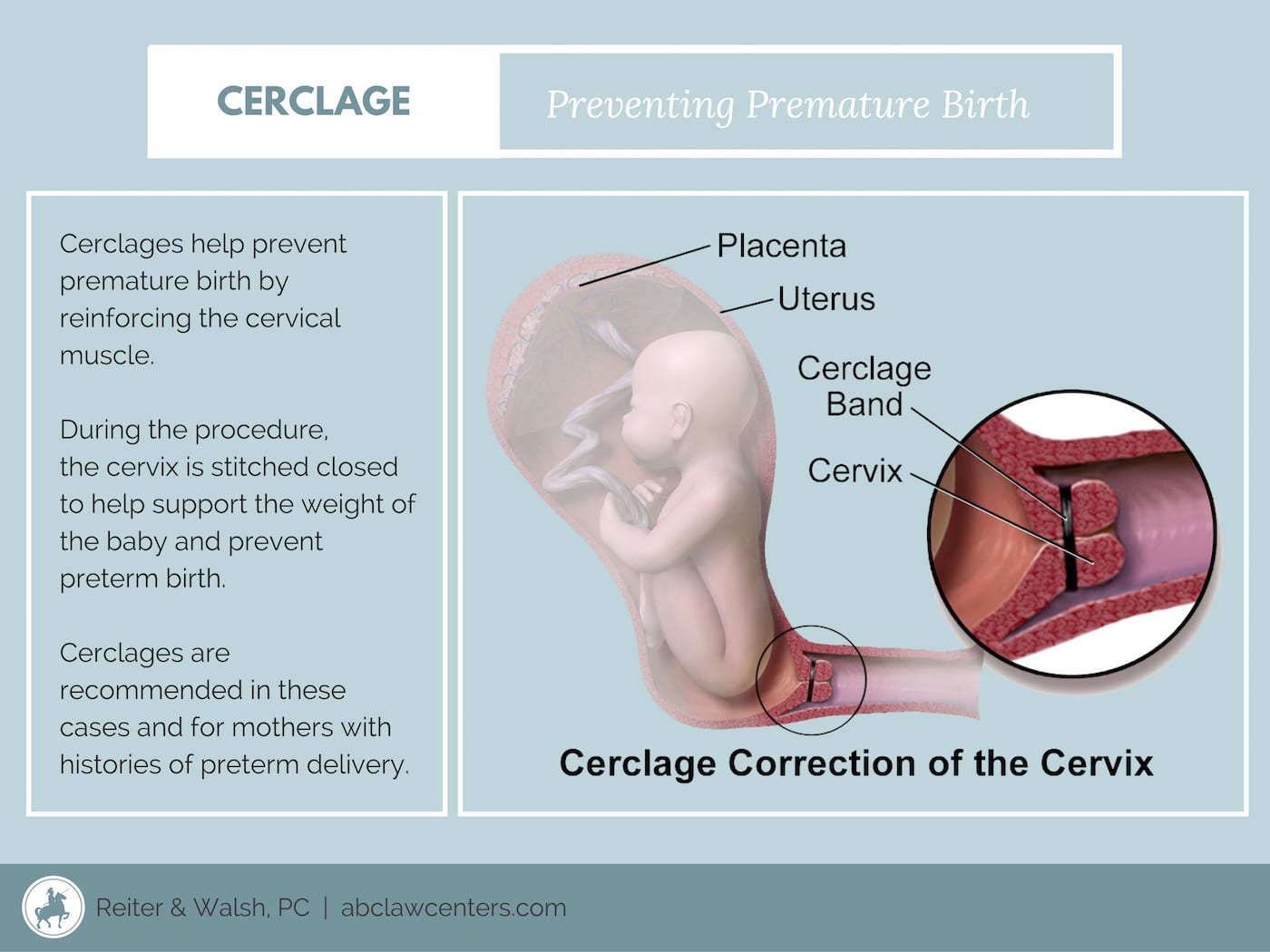
Cervical cerclage
A cervical cerclage is a stitch or tape placed in the cervical tissue to help keep the cervix closed (2). Medical professionals use transvaginal ultrasounds to determine the cervical length and recommend cervical cerclage based on their findings. Cerclage can help relieve some of the pressure on weakened cervical tissue and help the pregnancy last longer.
Cerclages can also reduce the risk of an ‘ascending infection’ – an infection that ascends from the vagina into the upper genital tract. The cervix acts as a physical barrier between the vagina and the upper genital tract, and a cerclage can help maintain the barrier’s integrity. Cerclages are removed typically around the 37th week of pregnancy, or earlier if the mother goes into preterm labor (8).
Progesterone
Progesterone is a hormone that has many purposes in the body and is very important during pregnancy. It can help avert preterm birth by modulating inflammatory responses – one of the factors that can lead to early labor (9). It also inhibits cervical ripening and myometrial activity. Progesterone is given either as a vaginal suppository or injection.
Vaginal suppository progesterone is given to women with a short cervix, whether or not they’ve had a prior preterm birth. This treatment decreases the risk of (9):
- Respiratory distress syndrome (RDS) in the baby
- Low birth weight under 1500 grams
- NICU admission
- Need for mechanical intervention
This treatment is typically provided starting around 19-23 weeks and ends around 36 weeks.
Injected progesterone (17P) is given to women who have had a prior preterm delivery and is provided weekly. It is started around 14-16 weeks and administered once a week until around 26-36 weeks. This treatment reduces the risk of:
- Preterm birth
- Low birth weight
- Complications like IVH (intraventricular hemorrhage) and NEC (necrotizing enterocolitis)
- NICU admission
- Need for supplemental oxygen therapy
Some women benefit from the use of both cerclage and progesterone, particularly those with a prior preterm birth at less than 34 weeks, and with a current cervical length of less than 25 mm at less than 24 weeks’ gestation.
While cervical cerclage and progesterone are the only two approved treatments for prolonging pregnancy and preventing preterm birth, there are other methods that can be used to reduce the risk of injury in babies who are about to be born preterm.
Reducing the risk of injury in preterm babies
If a preterm birth is imminent and interventions do not stop it, there are two treatments that are given to the mother while the baby is still in-utero that help protect the baby’s brain and help mature the baby’s lungs. These treatments are antenatal steroids (one example is betamethasone) and magnesium sulfate.
Antenatal steroids (betamethasone)
Antenatal steroids are one of the most important therapies given to women before preterm birth to improve newborn outcomes (10). ACOG recommends that a single dose of antenatal steroids, betamethasone, be given to women between 24 to 34 weeks gestational age. Recent recommendations suggest offering them up to 36 weeks for these women if they have not previously received these steroids. They are given in two doses over 24 hours and are effective when given up to 4 months before birth. They are most effective, however, 1-7 days before birth. This treatment can benefit the baby in several ways (10):
- Accelerates lung maturity to decrease respiratory distress syndrome (RDS) rates
- Stabilizes the baby’s intracranial vasculature
- Decreases intraventricular hemorrhage incidence
- Decreases Periventricular leukomalacia incidence
- Decreases Necrotizing enterocolitis incidence
- Shortens preemie hospital stays
- Increases preemie survival rates
- Decreases inflammation rates
Magnesium sulfate
If a mother comes to the hospital with spontaneous preterm labor, she should be given magnesium sulfate to inhibit uterine contractions. This therapy also helps protect the fetal brain and improves long-term outcomes. This treatment decreases the rate of all severities of cerebral palsy, according to the BEAM Trial (11). This treatment is provided at a gestational age of fewer than 32 weeks if the mother has either:
- Active preterm labor with 4-8 cm cervical dilation (or Premature Rupture of Membranes, PPROM, after 22 weeks)
- Indicated preterm birth within 24 hours
Magnesium sulfate both protects babies’ brains and helps prolong pregnancy in the short-term.
The takeaway
If the risk factors for premature birth are properly managed, preterm birth and prematurity-related injuries can be avoided. Progesterone and cerclage can help avert preterm birth, while betamethasone and magnesium sulfate can improve outcomes in preemies. If medical professionals don’t take the proper actions to avert preterm birth and a baby is injured, parents can seek justice for their child.


Legal help for birth injuries
Physicians, nurses, midwives, and other medical professionals are obligated to do everything in their power to prevent premature birth. This includes diagnosing and treating its risk factors, preventing its causes, planning for delivery, calling necessary emergency C-sections, and providing all other means of care in accordance with a strict set of rules. The failure to properly handle or prevent premature birth is medical negligence, and when it causes injury, it is medical malpractice.
If you know of a child who experienced complications of premature birth, we encourage you to reach out to our birth injury, cerebral palsy, and premature birth lawyers today with your legal questions or case inquiries. ABC Law Centers: Birth Injury Lawyers is a niche law firm that specifically takes cases involving birth injury, so our attorneys have the specific skills, experience, and knowledge necessary to win these complex, multi-million dollar cases. While our team is based in Michigan, we handle cases all over the United States. The ABC Law Centers: Birth Injury Lawyers birth trauma team has also handled FTCA cases involving military medical malpractice and federally-funded clinics.
Contact our Michigan birth injury and premature birth lawyers today for a free legal consultation. We will review your case free of charge, determine the cause of your loved one’s injuries, and inform you of your legal options. We do not charge fees for any of our legal process unless we win!



Featured Videos
Posterior Position
Hypoxic-Ischemic Encephalopathy (HIE)

Featured Testimonial
What Our
Clients Say…
After the traumatic birth of my son, I was left confused, afraid, and seeking answers. We needed someone we could trust and depend on. ABC Law Centers: Birth Injury Lawyers was just that.
- Michael
Helpful resources
- Women’s Health Care Physicians. (n.d.). Retrieved March 5, 2019, from https://www.acog.org/Patients/FAQs/Preterm-Labor-and-Birth
- Newnham, J. P., Dickinson, J. E., Hart, R. J., Pennell, C. E., Arrese, C. A., & Keelan, J. A. (2014). Strategies to prevent preterm birth. Frontiers in immunology, 5, 584. doi:10.3389/fimmu.2014.00584
- Premature birth. (2017, December 21). Retrieved March 5, 2019, from https://www.mayoclinic.org/diseases-conditions/premature-birth/symptoms-causes/syc-20376730
- Premature Birth Complications: Risks of Complications. (2016, May 19). Retrieved March 5, 2019, from https://americanpregnancy.org/labor-and-birth/premature-birth-complications/
- Higuera, V. (n.d.). Premature Birth Complications. Retrieved March 5, 2019, from https://www.healthline.com/health/pregnancy/premature-baby-complications
- Amniocentesis. (2018, November 08). Retrieved March 8, 2019, from https://www.mayoclinic.org/tests-procedures/amniocentesis/about/pac-20392914
- Premature birth. (2017, December 21). Retrieved March 9, 2019, from https://www.mayoclinic.org/diseases-conditions/premature-birth/symptoms-causes/syc-20376730
- Cervical Cerclage: Benefits and Risks. (2016, July 15). Retrieved March 8, 2019, from https://americanpregnancy.org/pregnancy-complications/cervical-cerclage/
- https://www.uptodate.com/contents/progesterone-supplementation-to-reduce-the-risk-of-spontaneous-preterm-birth
- Women’s Health Care Physicians. (n.d.). Retrieved March 5, 2019, from https://www.acog.org/Clinical-Guidance-and-Publications/Committee-Opinions/Committee-on-Obstetric-Practice/Antenatal-Corticosteroid-Therapy-for-Fetal-Maturation?IsMobileSet=false
- Costantine, M. M., Weiner, S. J., Eunice Kennedy Shriver National Institute of Child Health and Human Development Maternal-Fetal Medicine Units Network (2009). Effects of antenatal exposure to magnesium sulfate on neuroprotection and mortality in preterm infants: a meta-analysis. Obstetrics and gynecology, 114(2 Pt 1), 354-64.