Signs of an Intrauterine Infection (Chorioamnionitis)
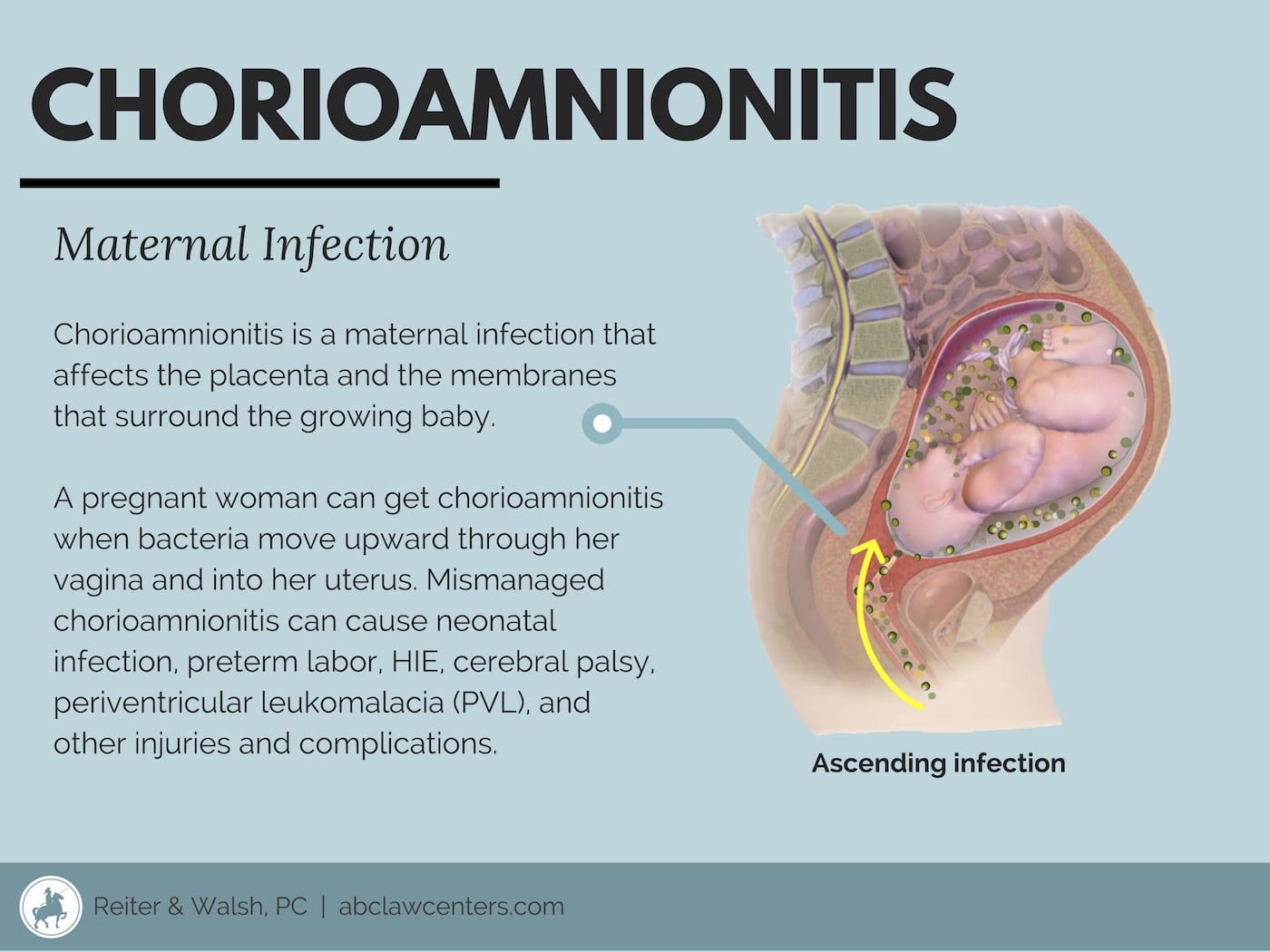
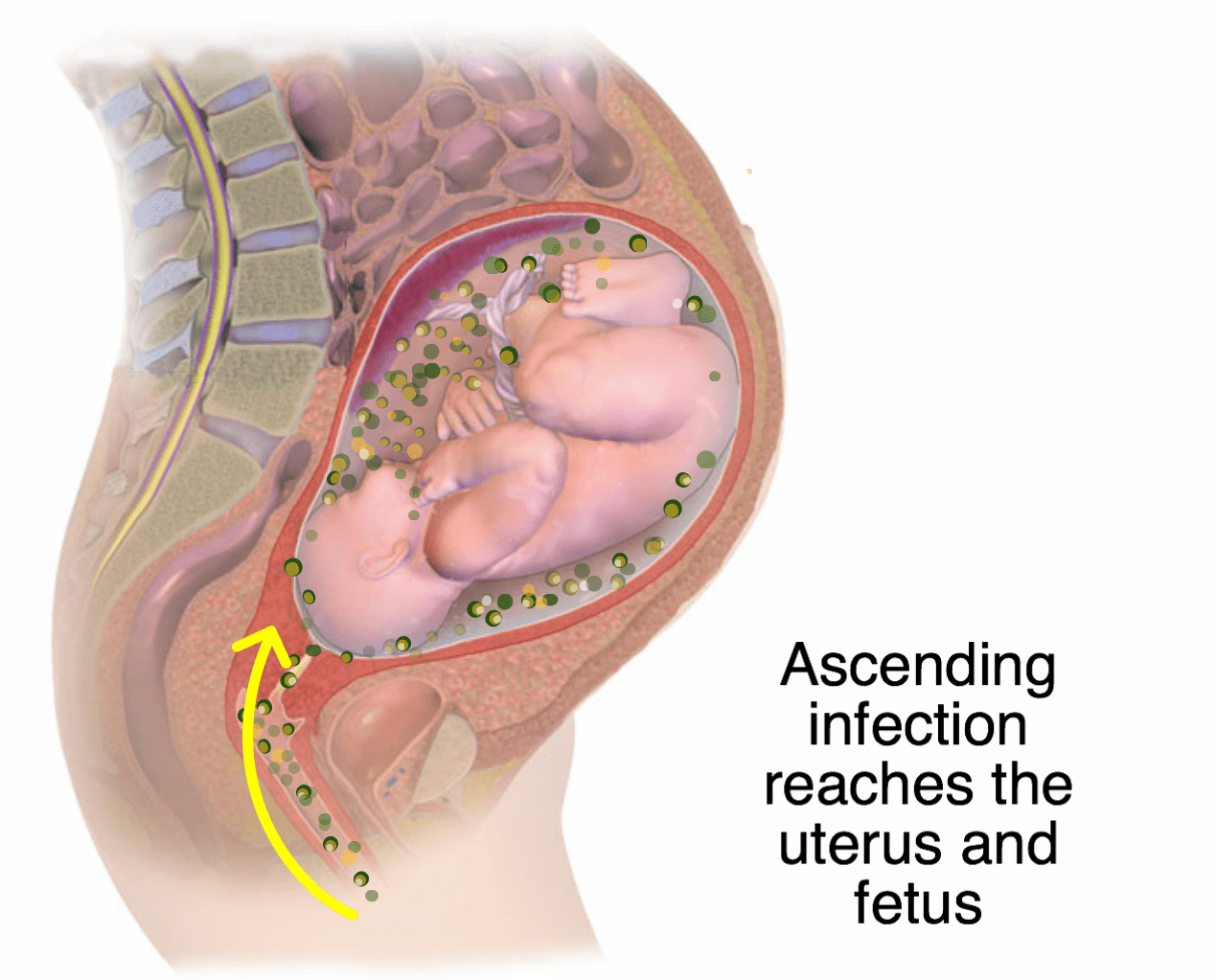
Chorioamnionitis is a pregnancy infection that affects the placenta and the membranes that surround the growing baby. A pregnant woman can get chorioamnionitis when bacteria move upward through her vagina and into her uterus. Chorioamnionitis can cause premature labor, and it can interrupt the exchange of nutrients and gases between the mother and baby. It can also spread to the baby through the umbilical cord or during vaginal birth. In most cases, chorioamnionitis is benign and does not cause harm.
In certain cases where chorioamnionitis is poorly managed, it can cause the baby to develop lifelong disabilities such as hypoxic-ischemic encephalopathy (HIE), cerebral palsy (CP), and periventricular leukomalacia (PVL). Doctors can prevent permanent harm through precautionary measures such as providing antibiotics to the mother and delivering the baby through an early, timely C-section (1).
Signs and symptoms of chorioamnionitis
Signs and symptoms may include the following (1):
- Maternal fever (this is the most important clinical sign of the infection)
- Diaphoresis (excessive sweating)
- Hypotension (low blood pressure)
- Uterine tenderness
- Significant maternal tachycardia (heart rate > 120 beats/min.)
- Fetal tachycardia (heart rate > 160 – 180 beats/min.)
- Purulent or foul-smelling amniotic fluid or vaginal discharge
- Maternal leukocytosis (high white blood cell count)
It is important to note that some women may exhibit no clear signs or symptoms of the infection.
Causes and risk factors
Chorioamnionitis, or intraamniotic infection, is usually caused by bacteria ascending into the uterus from the vagina or occasionally the colon. It is more likely to occur after premature rupture of membranes (PROM), which is when the amniotic sac and chorion rupture (also known as the “water breaking”) before the start of labor. Other risk factors for chorioamnionitis include (1):
- Premature labor
- Prolonged labor
- Nulliparity (no prior births)
- Group B streptococcus (GBS)
- Bacterial infections, such as urinary tract infection (UTI), bacterial vaginosis (BV), and ureaplasma
- Obesity during pregnancy
- Short cervix (incompetent cervix)
- Use of the hormone vaginal prostaglandin during labor
- Internal monitoring of labor
- Multiple vaginal exams
- Meconium-stained amniotic fluid
- Epidural anesthesia
- Immunocompromised status
- Smoking, alcohol, or drug abuse
Diagnosis
Chorioamnionitis may be diagnosed based on signs such as maternal fever, microbiological indications in amniotic fluid culture, or microscopic abnormalities in the umbilical cord and placenta.
A chorioamnionitis diagnosis is typically based solely on clinical signs, since access to uncontaminated amniotic fluid or placenta for culture is invasive and usually avoided. The presence of fever (temperature > 100.4) plus two other signs (uterine tenderness, maternal or fetal tachycardia, and foul/purulent amniotic fluid) is generally required for diagnosis. In addition, the presence of risk factors of chorioamnionitis, especially membrane rupture, further strengthens diagnosis (1).
Other diagnostic methods are listed below:
Laboratory tests for a mother with no symptoms and who is experiencing premature labor or PROM include:
- Examination of amniotic fluid
- Maternal GBS screening test
- Maternal blood studies
- Maternal urine studies
Testing of a febrile (feverish) mother with suspected chorioamnionitis includes:
- White blood cell counts
- C-reactive protein levels
- Alpha 1-proteinase inhibitor complex measurement
- Serum interleukin-6 or ferritin levels
Studies to evaluate amniotic fluid and urogenital secretions include:
- Bacterial cultures
- Leukocyte count
- Gram staining
- pH
- Glucose concentration
Ultrasonography may be used to determine the wellbeing of the baby in the womb.
Tell us your story.
A diagnosis after a poorly managed intrauterine infection is difficult. Our team at ABC Law Centers: Birth Injury Lawyers is here to answer your questions and help secure your family’s future.
Prevention
Preventing chorioamnionitis is critical. Premature rupture of membranes (PROM) and premature preterm rupture of membranes (PPROM) are major causes of chorioamnionitis; up to 70% of women who develop PROM with contractions or labor have chorioamnionitis. Although PROM can cause chorioamnionitis, it must be noted that together with preterm labor, PROM may also be caused by chorioamnionitis.
Standard of care for preventing chorioamnionitis includes the administration of broad-spectrum antibiotics, typically involving erythromycin or azithromycin, and ampicillin for 7-10 days via IV (2 days) followed by oral routes (1). Additionally, labor induction and delivery is associated with reduced maternal infection and reduced need for neonatal intensive care. When there is prolonged membrane rupture (> 18 hours) at term, prophylactic antibiotics are not indicated if the mother is not colonized with GBS. However, the Centers for Disease Control (CDC) recommends initiating GBS prophylaxis if GBS status is unknown (2).
Indeed, prophylactic antibiotics have been shown to be very beneficial in reducing the incidence of neonatal death, chronic lung disease, or major brain abnormalities in the baby. Antibiotics also have been shown to reduce the incidence of chorioamnionitis and neonatal sepsis (infection of the bloodstream), and to prolong time-to-delivery among mothers with preterm membrane rupture who are given expectant management (waiting for spontaneous labor).
Treatment
Treatment for a mother and baby with chorioamnionitis includes early delivery, supportive care, and antibiotic administration.
Prompt administration of antibiotics is essential to prevent both maternal and fetal complications. Time to delivery after implementing antibiotic therapy has been shown to not affect morbidities, in certain cases. Thus, C-section to expedite delivery is not indicated for chorioamnionitis unless there are other obstetric indications. Intravenous (IV) administration of ampicillin every 6 hours and gentamicin every 8-24 hours until delivery is the standard regimen (1). If C-section is performed, clindamycin every 8 hours (or metronidazole) usually is added for anaerobic coverage. Treatment also should include administration of an additional IV dose of antibiotics after delivery (1).
Supportive measures include the use of acetaminophen (Tylenol), which is especially important during delivery to prevent neonatal encephalopathy (brain damage) (1).
Possible Issues Caused by Untreated Chorioamnionitis
Chorioamnionitis is very common and typically doesn’t harm the mom or baby. Occasionally, it can damage the membranes, as well as cause release of the hormone prostaglandin and cervical ripening, which may result in early labor. Additionally, the inflammation may spread to the chorionic villi, which cover the placenta and facilitate the exchange of nutrients and gases between the mother and baby. This is a condition called villitis, which is usually benign but can increase the risk of fetal death.
If chorioamnionitis and/or villitis are not properly treated, it can infrequently lead to serious outcomes in the baby, including:
- Hypoxic-ischemic encephalopathy (HIE)
- Hydrops fetalis (abnormal amounts of fluid build-up in two or more body areas of a fetus or newborn)
- Intrauterine growth restriction (IUGR)
- Respiratory problems
- Cerebral palsy
- Periventricular leukomalacia (PVL)
- Neonatal sepsis and meningitis
What is funisitis?
Funisitis is inflammation of the umbilical cord in response to the umbilical cord becoming infected. Funisitis often results from chorioamnionitis when the infection spreads from the placental membrane to the umbilical cord, causing fetal inflammatory response syndrome (FIRS). Funisitis is usually benign, but can occasionally cause the flow of oxygen and nutrients to the baby to become compromised when delivery is not timely.


Legal help for chorioamnionitis
If your child had chorioamnionitis and now has a serious condition such as hypoxic-ischemic encephalopathy or cerebral palsy, there is a possibility that they received improper medical care. You may want to consider pursuing a medical malpractice lawsuit.
At ABC Law Centers: Birth Injury Lawyers (Reiter & Walsh, P.C.), we are dedicated to birth injury cases (which include infection and oxygen deprivation). Our award-winning attorneys understand the complex legal issues involved with pregnancy infection and will help you to obtain the compensation to which you are entitled.



Featured Videos
Posterior Position
Hypoxic-Ischemic Encephalopathy (HIE)

Featured Testimonial
What Our
Clients Say…
After the traumatic birth of my son, I was left confused, afraid, and seeking answers. We needed someone we could trust and depend on. ABC Law Centers: Birth Injury Lawyers was just that.
- Michael
Helpful resources
- Tita, A. T. (2018, August). Intra-amniotic infection (clinical chorioamnionitis or triple I). Retrieved from https://www.uptodate.com/contents/intra-amniotic-infection-clinical-chorioamnionitis-or-triple-i?search=chorioamnionitis treatment&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1#H18.
- Horsley, E. (2011, May 01). CDC Updates Guidelines for the Prevention of Perinatal GBS Disease. Retrieved from https://www.aafp.org/afp/2011/0501/p1106.html.