Improper Fetal Monitoring and Birth Injury
Fetal heart monitoring is the best way for medical professionals to tell whether a baby is getting enough oxygen. If the baby’s heart rate is too high (tachycardia), too low (bradycardia), or otherwise abnormal, this is a sign of fetal distress. Fetal distress can mean that the baby’s body is trying to compensate for oxygen-depriving conditions; it is considered a medical emergency and should be promptly addressed. Fetal distress/an abnormal heart rate could be caused by a chronic (long-lasting) issue such as uteroplacental dysfunction or an acute (short-term) issue like uterine tachysystole/hyperstimulation. Both of these are very serious problems. If medical professionals fail to use fetal heart rate monitors as indicated, use monitors incorrectly, improperly interpret monitor readouts, or fail to intervene when necessary, the consequences could be serious. If the baby is harmed by negligent actions related to fetal heart rate monitoring, this constitutes medical malpractice.
Understanding fetal heart rate
There are certain heart rate ranges in unborn babies that can indicate their health status. Please note that different organizations promote different guidelines; the following ranges came from a literature review published by UpToDate (1):
- Normal fetal heart rate (or ‘baseline’): approximately 110 – 160 beats per minute
- Slow fetal heart rate (bradycardia): under 110 beats per minute
- Fast fetal heart rate (tachycardia): more than 160 beats per minute.
What is considered to be a healthy fetal heart rate can vary somewhat depending on the baby’s gestational age (2).
If a baby has an abnormal heart rate and is not close to term, medical professionals screen them for intrauterine growth restriction (IUGR) and other complications that can reduce oxygen flow to the baby, resulting in adverse outcomes. Medical professionals may suggest a variety of tests, including (1):
- Biophysical profile (BPP)
- Nonstress test
- Assessment of amniotic fluid volume
- Doppler velocimetry (to examine blood flow in the placenta)
- Maternal tests for uteroplacental circulation problems
What does it mean when fetal heart rate is high (tachycardia)?
There are several causes of a fast fetal heart rate (tachycardia), including hypoxia (oxygen deprivation), maternal fever, amniotic fluid infection, and more.
Fetal tachycardia can mean that the baby’s heart is working harder than normal to pump blood and oxygen to the rest of the body. This is a compensatory mechanism that can help offset low oxygen conditions (to some degree). However, this compensatory mechanism fails after a certain time period because babies are not capable of maintaining such a fast heartbeat. Sustained tachycardia puts babies at risk for cardiovascular failure. It can also be a sign of nonimmune hydrops fetalis (3), which is a dangerous excess of fluid in fetal soft tissues and serous cavities (4). It is very important that medical professionals do all they can to prevent cardiovascular failure and hydrops fetalis in babies showing signs of fetal tachycardia. This may involve expectant management, medical treatment, or an early delivery.
What does it mean when fetal heart rate is slow (bradycardia)?
A slow fetal heart rate (bradycardia) can be caused by a number of factors. In many cases, it results from fetal oxygen deprivation caused by dangerous complications such as uterine tachysystole/hyperstimulation, placental abruption, or uterine rupture (5). It can also be caused by maternal health issues, such as hypotension or seizures (3).
If the bradycardia is due to fetal distress (oxygen deprivation), the baby should be delivered right away, usually by emergency C-section.
Fetal heart rate during labor
During labor, fetal heart rate is monitored using electronic fetal monitoring to see if the baby is tolerating contractions well.
If the baby’s heart rate is abnormally fast, slow, or otherwise abnormal, this could be a sign that the baby is in distress (being deprived of oxygen). Despite the standard use of fetal monitoring in hospitals today, sometimes doctors and nurses still fail to monitor their patients or improperly interpret monitor tracings. This can lead to debilitating birth injuries for the baby, including brain damage.
During labor, the baby’s heart rate should be ‘variable’ (it rises and falls, showing as a jagged line on the monitor). Good variability indicates a healthy cardiac and circulatory system. A baby’s heart rate is said to be “reassuring” if the fetal heart rate pattern has normal variability with accelerations and normal baseline. This usually means that the baby is well oxygenated and is tolerating labor and delivery well (1).
If the baby’s heart rate does not rise and fall as expected or begins to flatten out, variability is said to be minimal or absent, and the underlying cause needs to be found. Babies whose heart rates aren’t variable may be having issues with decreased oxygenation; this is an emergency.
There are some interventions that can help the baby’s heart rate and increase oxygenation to the baby. These include (5):
- Changing the mother’s position
- Administering oxygen to the mother
- Providing the mother with IV fluids
- Stimulating the fetal scalp (this may accelerate the fetal heart rate)
- Doing an amnioinfusion
- Reducing uterine contraction frequency (by decreasing/stopping contraction-enhancing medications such as Pitocin and Cytotec, which can lead to uterine tachysystole/hyperstimulation)
However, C-section is often the best and fastest way to handle fetal heart rate abnormalities. In utero, there are limited options for helping treat a baby in distress. Once the baby is born, medical professionals can initiate resuscitation procedures and other medical interventions that can help remediate the in-utero conditions that caused the fetal distress.
Fetal monitoring and birth injury prevention
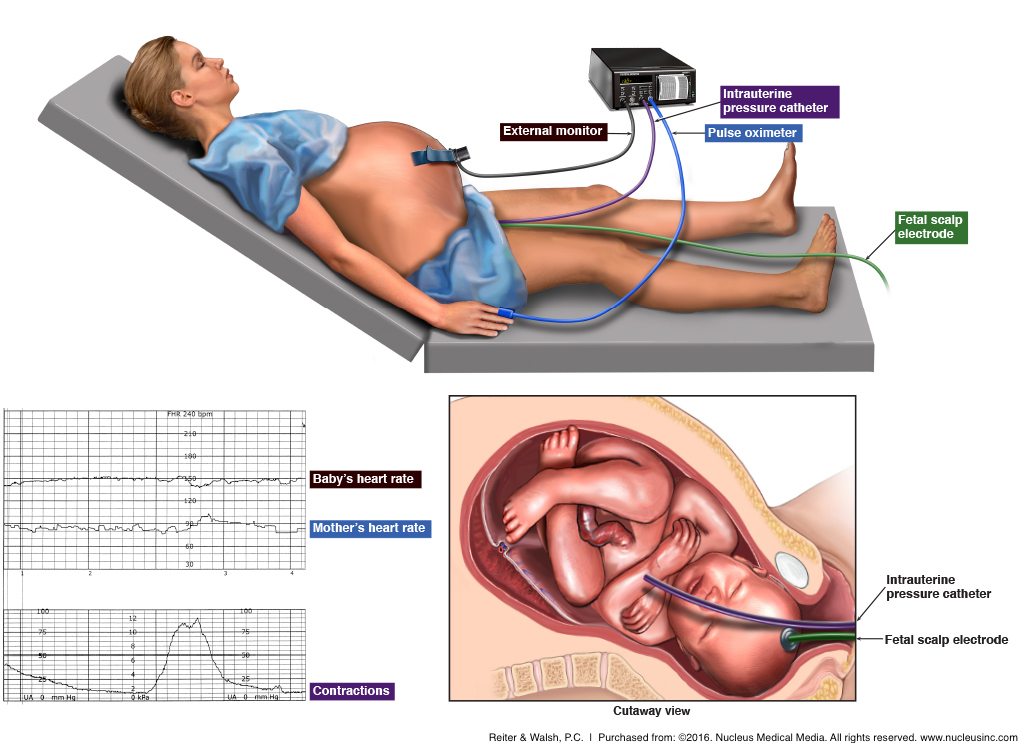
There are two methods of fetal monitoring: external and internal. External monitoring can be done either periodically or continuously. Periodic external monitoring is called auscultation, and it involves the use of a transducer, which is placed on the mother’s abdomen. This may be done in low-risk pregnancies – high-risk pregnancies necessitate continuous monitoring.
Many women have electronic fetal monitoring (EFM) which records the baby’s heart rate in response to contractions. This is accomplished by strapping a belt-like device around the mother’s abdomen.
Internal monitoring involves attaching an electrode to the baby’s scalp (this is only possible once the fetal membranes have ruptured, i.e., the mother’s water has broken). The internal fetal monitor may provide a more accurate measurement of the baby’s heart rate and the mother’s contractions than the external monitor (6). In both methods, the data is transferred through the wires on the monitors to a machine that records and prints the information on strips for doctors and nurses to read.
During labor, when a mother has a contraction, the baby’s heartbeat will drop slightly (this is called a deceleration), but should return to normal once the contraction is over. The fetal monitoring strip shows any discrepancies in this pattern. For example, if the monitor shows that a baby’s heart rate does not recover immediately after the contraction, or if there is a deceleration in the baby’s heart rate starting at the peak of the contraction or right after the contraction (a “late” deceleration), or there are too many decelerations which are too deep, there may be a problem with the baby (7).
Signs and symptoms of fetal distress (non-reassuring heart tracings)
A heart rate greater than 160 (tachycardia), a heart rate lower than 110 for an extended period of time (bradycardia), a decrease in fetal heart rate variability, an abnormal severity or frequency of variable decelerations, or late returns to baseline heart rate are considered “non-reassuring” indications (1, 7). In some cases, non-reassuring heart tracings signal that the baby is not getting enough oxygen and if not delivered soon, could suffer birth asphyxia (hypoxic-ischemic encephalopathy).
Fetal distress and birth injuries: causes
There are a number of serious conditions that can occur during labor and delivery and cause the fetal heart rate to become non-reassuring. Some of these include:
- Uterine tachysystole (labor contractions are too strong, too long, or too frequent). Sometimes this can occur as a result of labor induction medications such as Pitocin (synthetic oxytocin) and Cytotec.
- Umbilical cord problems like umbilical cord compression, umbilical cord prolapse (umbilical cord precedes the baby’s exit from the uterus), or nuchal cord (cord wrapped around baby’s neck).
- Placental abruption (placenta separates from the uterine wall).
- Uterine rupture (a tear in the wall of the uterus, usually at the site of a previous c-section incision).
- Uteroplacental insufficiency (insufficient amount of blood flowing to the placenta).
- Polyhydramnios (excessive amniotic fluid) or oligohydramnios (insufficient amniotic fluid)
- Cephalopelvic disproportion (baby’s head is too big to fit through mother’s pelvis), macrosomia (large baby), breech (baby is positioned in a buttocks or foot-first position instead of head-down), or other delivery complication that causes the baby to get caught in the birth canal.
Classifying normal and abnormal fetal heart rates in labor and delivery
During labor and delivery, fetal monitoring is used to:
- Ensure the baby has enough oxygen
- Reduce the risk of neonatal complications due to oxygen deprivation.
Professionals use electronic fetal heart rate monitoring to spot signs of fetal hypoxia and intervene appropriately to eliminate or reduce the risk of HIE and other birth injuries.
In 2008, experts proposed a three-category system for classifying fetal heart rate (FHR) tracings. The system divides fetal heart rate tracings into three categories (8):
- Category I Fetal Heart Tracings: Category I fetal heart rate tracings are considered normal. These tracings include all of the following:
- A baseline FHR between 110-160 beats per minute
- A moderate level of baseline FHR variability (meaning that the
- FHR waivers only moderately from the baseline level)
- Absence of late or variable decelerations
- Presence or absence of both FHR accelerations and early decelerations
- Category II Fetal Heart Tracings: Category II fetal heart rate tracings are considered ‘indeterminate.’ Some characteristics of Category II tracings are considered benign, while others are more urgent and may require prompt interventions to avoid brain injury due to oxygen deprivation. Some of the qualities of category II fetal heart rate tracings are:
- Bradycardia (when there is baseline FHR variability)
- Tachycardia
- Minimal or marked baseline variability
- Absent baseline variability with no recurrent FHR decelerations
- Absence of induced accelerations in FHR after stimulation of the baby
- Category III Fetal Heart Tracings: Category III fetal heart rate tracings are considered abnormal and require appropriate intervention, which often includes prompt delivery, often via emergency C-section. If
- Category III fetal heart rate tracings are allowed to continue without intervention, this will likely result in fetal brain injury. Category III tracings include either:
- Absent baseline variability (with recurrent late decelerations, recurrent variable decelerations, or bradycardia), or
- Sinusoidal pattern (a pattern that appears as a smooth, repeating wave, but does not resemble a normal FHR pattern)
The pitfalls of the three-category EFM classification system
Because the three-category system of classification includes a broad Category II section, some researchers find that this system is less useful for providing medical professionals with guidelines for intervening when concerning heart rate tracings show up. Some researchers have suggested more granular classification systems, providing medical professionals with more precise categories for various heart rate tracing patterns (9).
Fetal heart rate monitoring is a critical tool for understanding how a baby is tolerating labor. If medical professionals do not act on concerning fetal heart rate tracings, they are putting the baby at risk of injury. During labor and delivery, a well-trained and experienced medical staff member should be watching the fetal monitoring strips for concerning signs and intervene (which may involve alerting additional staff members) if necessary. If they do not, it is medical malpractice, because their actions increase the baby’s chances of being injured by oxygen deprivation.


Legal help for fetal monitoring errors, HIE, and birth injury
The sole purpose of the fetal heart monitor is to allow medical staff to identify any signs of fetal distress and to take swift and appropriate action. If a healthcare provider ignores or misinterprets the fetal monitor strips, resulting in oxygen deprivation and brain damage, it is medical malpractice. Birth injury cases require specific, extensive knowledge of both law and medicine. In order to achieve the best results, our team believes it’s critical to specifically and exclusively handle birth injury cases.
Our firm, which is based in Detroit, Michigan, has helped families across the United States in cases involving fetal monitoring errors, delayed delivery, and other birth injuries and complications. Our team has also handled FTCA (Federal Tort Claims Act) cases involving military medical malpractice and federally-funded clinics.



Featured Videos
Posterior Position
Hypoxic-Ischemic Encephalopathy (HIE)

Featured Testimonial
What Our
Clients Say…
After the traumatic birth of my son, I was left confused, afraid, and seeking answers. We needed someone we could trust and depend on. ABC Law Centers: Birth Injury Lawyers was just that.
- Michael
Helpful resources
For more information on fetal heart rate monitoring, please see the American Academy of Family Physicians’ Guide to EFM.
- (n.d.). Retrieved from https://www.uptodate.com/contents/intrapartum-fetal-heart-rate-assessment
- Weerakkody, Y. (n.d.). Fetal heart rate | Radiology Reference Article. Retrieved from https://radiopaedia.org/articles/fetal-heart-rate
- (n.d.). Retrieved from https://www.uptodate.com/contents/overview-of-the-general-approach-to-diagnosis-and-treatment-of-fetal-arrhythmias
- (n.d.). Retrieved from https://www.uptodate.com/contents/nonimmune-hydrops-fetalis
- (n.d.). Retrieved from https://www.uptodate.com/contents/image?imageKey=OBGYN%2F71679&topicKey=OBGYN%2F418&source=outline_link
- Fetal Monitoring: External and Internal Monitoring. (n.d.). Retrieved from https://www.healthline.com/health/pregnancy/external-internal-fetal-monitoring#3
- Fetal Heart Monitoring: What’s Normal, What’s Not? (n.d.). Retrieved from https://www.healthline.com/health/pregnancy/abnormal-fetal-heart-tracings
- Macones, G. A., Hankins, G. D., Spong, C. Y., Hauth, J., & Moore, T. (2008). The 2008 National Institute of Child Health and Human Development workshop report on electronic fetal monitoring: update on definitions, interpretation, and research guidelines. Journal of Obstetric, Gynecologic, & Neonatal Nursing, 37(5), 510-515.
- Parer, J. T., Ikeda, T., & King, T. L. (2009). The 2008 National Institute of Child Health and Human Development report on fetal heart rate monitoring. Obstetrics & Gynecology, 114(1), 136-138.