Brain Imaging and HIE: A Comprehensive Overview
The Importance of Neonatal Brain Imaging to Diagnose HIE
- Neonatal encephalopathy (NE) is a brain injury that causes a baby to have signs and symptoms of brain dysfunction.
- Hypoxic-ischemic encephalopathy (HIE) is a brain injury caused by a lack of oxygen (hypoxia) and/or a lack of blood flow (ischemia) to the brain.
Magnetic resonance imaging (MRI) is the preferred imaging method for diagnosing neonatal brain injury. Studies using MRI techniques show that most cases (over 75%) of NE are caused by HIE brain injury that occurs during or near the time of birth. Certain signs during this period are high indicators that a brain injury occurred. For example, swelling due to excess fluid in the brain (edema) may be a warning sign.
It is very important to recognize NE and HIE as soon as possible. In cases of HIE, hypothermia treatment must be given within 6 hours of the oxygen-depriving incident. This cooling treatment helps to limit the cycle of brain injury and prevent death and long-term conditions such as cerebral palsy.
Diagnosing HIE and neonatal brain damage promptly is critical in preserving a baby’s ability to have an improved outcome from a birth injury.
If you have questions about your baby’s future, reach out to an experienced birth injury lawyer today. Our team is ready to hear your story and help you to understand your legal options.
Understanding Hypoxia vs. Ischemia
When there is a hypoxic-ischemic insult to the baby’s brain, the injury can evolve over a period of days and weeks.
Hypoxia is a lack of oxygen.
Ischemia is a restriction of blood flow.
Both cause cell injury and brain damage, and they are not mutually exclusive.
However, ischemia contributes more significantly to brain injury. Global ischemia causes cellular energy failure. It also causes a build-up of acids and other toxins that harm cells in a number of ways, mainly by making it more difficult for cells to receive oxygen.
Certain parts of the brain are more vulnerable to hypoxic-ischemic injuries than others. The location and extent of the brain injury depend on:
- The severity of the condition
- The length of time without oxygen or blood flow
- the condition of the fetus (fetal reserve)
Hypoxic-Ischemic Injury Timeline
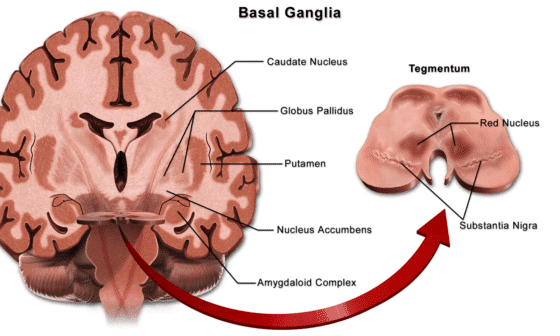
The Basal Ganglia
Listed below is a timeline of some significant events that occur when the brain suffers from a lack of oxygen-rich blood. The events may not occur with all types of hypoxic-ischemic injuries.
For example, injury to the basal ganglia may occur with profound (near total) asphyxia and mixed injury patterns. The basal ganglia may not be affected by a partial prolonged insult.
TIMELINE
0 – 12 hours after hypoxic-ischemic insult (HII)
- prominent involvement of the basal ganglia
- focal cerebral infarction (tissue death)
- focal cerebral lesions.
12 – 24 hours after HII
- basal ganglia damage occurs.
24 – 36 hours after HII
- Major cell changes
- observable cell swelling.
24 – 72 hours after HII
- Signs of swelling
- edema (fluid build up)
- typically is increased ICP.
72+ hours after HII
- selective neuronal necrosis involving:
- basal ganglia
- thalamus
- brain stem
Brain Imaging, HIE, and Medical Negligence

Medical staff must recognize when a baby is not getting enough oxygen on fetal monitoring and deliver before a baby suffers HIE. Health systems must also detect brain injury and diagnose HIE as quickly as possible. Early intervention is critical in minimizing the effects of a hypoxic-ischemic incident.
Brain imaging studies help clinicians determine if asphyxia caused the brain injury. These studies also help pinpoint the timing of the brain injury.
If a brain injury was preventable, the hospital and medical professionals should be held accountable.
A child with HIE will need specialized therapy and treatment. The child may have unique housing and educational needs as they grow. The costs of care may become expensive and draining for parents and caregivers.
In situations with medical negligence, a lawsuit can help families afford the care their child deserves. At ABC Law Centers, we focus exclusively on these complex birth injury cases. Call us today for a free consultation. Our team is here to help you.
Types of HIE Brain Injury Patterns
Acute Near Total / Acute Profound Asphyxia
When the baby suffers severe or near total hypoxia or birth asphyxia, the insult is called acute/profound asphyxia or profound (near total) asphyxia.
With very severe insults to the brain, there will usually be a central pattern of injury in a specific spot. A focal neuronal injury (deep gray matter injury) affects many levels of the central nervous system. This kind of injury will also involve noticeable death of brain cells.
- When the insult is relatively abrupt and severe, there will be an injury to the deep nuclear brain structures, such as: the basal ganglia
- thalamus
- brainstem
Shunting during acute profound asphyxia
Deep brain structures are more vulnerable to abrupt and severe insults usually lasting 10 to 25 minutes. This is because total asphyxia prevents the adaptive mechanism of shunting blood to vital areas of the brain. Consequently, the cerebral cortex of the brain will typically be spared from injury.
When a baby suffers severe and prolonged oxygen deprivation or ischemia, there is a cerebral deep pattern. There might be at least some degree of shunting. These types of insults usually cause damage to the cerebral cortex and deep structures, especially the basal ganglia, putamen, and thalamus.
Causes of acute profound asphyxia
Placental abruption, uterine rupture, prolapsed umbilical cord and terminal bradycardia (slow heart rate) are examples of conditions that can cause acute profound asphyxia.
Partial Prolonged Asphyxia
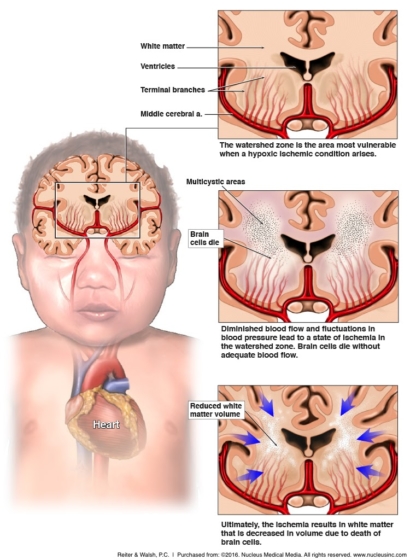
Partial prolonged asphyxia incidents usually last for more than 30 minutes to hours. These injuries mainly lead to cortical injury in the watershed and parasagittal white matter regions. Relatively speaking, the deep gray matter is spared from damage.
The cerebral cortex – the outermost layer of neural tissue – is also vulnerable to prolonged, less severe hypoxia/ischemia. When the brain suffers these conditions, blood gets shunted away from the cerebral cortex to the deeper structures of the brain. The watershed regions are also vulnerable to injury. These areas do not have a direct arterial blood supply.
Causes of partial prolonged asphyxia
Partial prolonged asphyxia can be caused by Pitocin and Cytotec use. Pitocin and Cytotec are labor induction drugs that can cause contractions to be too strong, too long, or too frequent. During these kinds of contractions, the blood vessels in the placenta are almost continuously restricted. The constricted blood vessels cause a decrease in the amount of oxygen-rich blood going to the baby.
Other events that can cause partial prolonged asphyxia include:
- hypertension
- hypotension
- umbilical cord compression, caused by a nuchal cord or oligohydramnios (too little amniotic fluid)
- placental insufficiency
- inadequate or delayed resuscitation of the baby at birth.
Mixed Injury Pattern
There also can be a mixed injury pattern. This result indicates the baby experienced both profound asphyxia and partial prolonged asphyxia.
Progression of Brain Injury: A Cellular View
When the oxygen saturation in the baby’s blood drops, the brain may not be affected initially. However, when the oxygen supply gets too low, hypoxia develops.
Hypoxia
Hypoxia results in anaerobic metabolism. Anaerobic metabolism is the creation of energy in the absence of oxygen.The build-up of acids (acidosis) created by this process has a direct, harmful effect on neurons (brain cells).
Acidosis and Ischemia
Acidosis also can lead to a drop in fetal blood pressure. Lowered blood pressure causes a reduced flow of blood in the brain, which leads to ischemia.
Both hypoxia and acidosis cause reduced blood flow to the baby’s brain. Research shows that hypotension and resultant diminished brain perfusion are significant factors associated with neuronal injury and HIE.
Effects of Reperfusion Injury (Secondary Brain Injury) During Hypoxic-Ischemic Phase
The brain damage that occurs during this hypoxic-ischemic phase is worsened by a reperfusion injury. A reperfusion injury is a secondary injury that occurs 2 – 6 hours later. As blood flow in the brain is restored, there is an increase in oxygen in the blood. The increased oxygen leads to free radical production that causes further cell damage, energy failure, and more brain injury.
Cell Death
When HIE occurs, some neurons always die. All the cells in the brain can be affected by HIE, but the neurons are the most vulnerable. Neurons process and transmit information via electrical and chemical signals. They connect to each other and form the core of the nervous system.
On a cellular level, each individual neuron can have a selective degree of injury. If a neuron – or any cell – does not get the oxygen and glucose it needs, it cannot produce energy for cell functions. Energy depletion leads to cellular injury or traumatic cell death (neuronal necrosis).
Apoptotic Cell Death
Sometimes, cells die through a process called apoptotic cell death. When a brain cell is significantly injured, it begins a programmed process called apoptosis. This series of events leads to cell death. The apoptotic cell death process occurs hours to days after the initial hypoxic-ischemic injury.
Brain Imaging Techniques and Injury Diagnosis
Diagnosing HIE Using MRI
Magnetic resonance imaging (MRI) is the best imaging technique for diagnosis of babies with moderate to severe HIE. MRIs can be performed 12 – 24 hours to days after birth. Edema and injury are usually evident by 24 hours on MRI or sooner.
During an MRI, images are taken from several angles:
- the top of the skull down to the base
- from the front to back
- from side to side.
Each image represents a unique slice of the brain. All areas of the brain are captured so that each layer can be analyzed.
High signal areas are areas of abnormal tissue (lesions). When the brain is damaged, a scar forms over the injury. Lesions and scarring give off a high signal. This hyperintense signal differentiates injured tissue from normal tissue.
MRI can accurately demonstrate the injury pattern one day after birth, sometimes sooner. The hyperintense area appears especially after day 4 of the baby’s life.
Diffusion-weighted Imaging (DWI)
Diffusion-weighted imaging (DWI) allows identification of injury in the first 24 – 48 hours. This sequence can show swollen and injured areas in the brain. DWI changes peak at 3 – 5 days of life. These changes may underestimate the extent of the damage, because the apoptotic cell death process takes a longer time to show the final extent of the injury.
MRI Patterns of Hypoxic-Ischemic Injuries
Generally, hypoxic-ischemic injuries show a 1, 2, 3, 4 sign on MRI:
- Increased signal intensity in the basal ganglia;
- Increased signal intensity in the thalamus;
- Absent or decreased signal intensity in the posterior limb of the internal capsule (white matter structure that carries information past the basal ganglia);
- Restricted water diffusion on diffusion-weighted images.
Profound (Near Total) Asphyxia on MRI
Typically, a newborn baby’s acute profound injury can be seen on MRI by 24 hours. The major effects of edema resolve by the end of day 5 or the beginning of day 6.
Significant edema in the central gray matter structures will show compression of the third ventricle. This injury affects the thalami and basal ganglia.
A more extensive injury that involves the rolandic cortex will show compression of other ventricular areas as well. This injury affects the motor area of the cerebral cortex.
After 72 hours, compression of the ventricles may increase, depending on how extensive the injury process is. When the injury process is on day 3, going until day 6, compression of the ventricles resolves, and they go back to their regular size.
The increased signal intensity sometimes changes with the initial evolution of damage. Sometimes there is no change to signal intensity.
Once swelling goes down and injured tissue remains, this alone can cause changes in signal intensity.
As the cycle of injury continues over weeks to months, the changes are best shown when the child is 18 months of age or older. The scarring, or gliosis, will contrast on the MRI. Atrophy after the injury will cause a decrease in tissue volume. The cerebral spinal fluid-filled spaces become abnormally large. The injury also leads to localized softening of brain tissue, which becomes more evident over time.
Partial Prolonged Asphyxia on MRI
Injuries in the watershed zones are typically gradual in onset and can involve both gray and white matter. These injuries are typically seen within 24 hours or later.
As edema increases, the cortex will become less dense. There will be less differentiation between gray and white matter. This loss often involves either the parietal-occipital lobes, frontal lobes, or both.
Injuries in the watershed zones can be in different areas:
- on one side of the brain
- more through the middle of the brain
- anterior
- posterior
Damage Beyond Watershed Zones
When the partial prolonged asphyxia lasts longer, the damage can extend beyond the watershed zones, into the adjacent cortical areas. This causes major edema, leading to the destruction of much of the lateral ventricles.
Brain swelling is greater than what it was at 24 hours, peaking at about 72 hours. Varying degrees of cerebral swelling can be seen at 36 hours and, to some extent, after 96 hours.
Watershed Injury Imaging Changes in the Cerebral Cortex
As edema subsides, the cortex will seem to appear again in the images at 8 days and later.This represents visualization of cortical necrosis. As tissue loss progresses, cystic and fluid-filled spaces completely replace areas of white and gray matter. The undersurface of a ridge on the cerebral cortex may have such compromised blood flow after the swelling that a mushroom-like structure appears beneath it. This structure appears after atrophy.
DWI is the best way to detect the earliest changes in watershed injury in partial prolonged asphyxia.
The damage will be seen as high signal intensity. Twenty-four hours after the hypoxic-ischemic insult, the cortex will lose its normal low signal intensity. The excess fluid causes increased brightness, making it indistinguishable from the bright white matter that is unmyelinated.
The excess fluid causes swelling in the white and gray matter, which compresses brain ventricles. As the edema subsides, cortical necrosis shows up as an increase in signal intensity. This high signal intensity disappears as the cortical reabsorption occurs. Cerebral volume loss will appear on the images. The volume loss may appear as cystic encephalomalacia, or the softening of brain tissue.
Gliosis
In response to a serious brain injury, the nervous system reacts with a process called gliosis. Gliosis produces a fibrous mass of cells called glial cells. These extra masses will appear as areas of increased signal intensity. Gliosis usually involves the subcortical white matter and cortex, and it can extend towards the ventricles within the white matter.
MRI Detection of Severe Injuries Beyond Watershed Regions
When partial prolonged asphyxia is severe, the brain injury can go beyond the typical watershed regions. The MRI detects a more extensive and homogenous pattern that includes edema and the effects of edema in large areas of all the cerebral lobes. This pattern will appear as increased intensity by 24 hours after the insult, and even sooner on DWI.
Maximal edema and subsided edema follow a similar time course as lesser degrees of partial prolonged asphyxia. Signs of cortical necrosis in the cortex show up as increased density on non-enhanced imaging and as abnormal increased signal intensity. These changes occur frequently in this severe type of situation.
As more and more fluid reabsorbs, cystic encephalomalacia and atrophy may occur. The ventricles and grooves on the brain structures are typically enlarged with additional collections of fluid outside of the brain.
Mixed Injury Patterns on Imaging
In mixed patterns, further injury can come in the form of near total collapse. Partial prolonged asphyxia depletes energy bases, which prevents cells from functioning.
This severe injury manifests when something causes the baby’s heart rate to suddenly slow (bradycardia) while the baby’s heart rate was already in a state of gradual decline. In addition to the injury from the partial prolonged asphyxia in the watershed zones or beyond, bradycardia causes further injury.
Severe bradycardic events can cause damage to the:
- putamen
- thalamus
- hippocampus
- vermis
- brainstem
The progression of mixed injuries is similar to the others described earlier.
Very severe near-total asphyxia may have the typical profound pattern of injury, but with greater extent of cortical injury. This is typically seen when the baby’s bradycardia is really long. This is a profound asphyxia injury pattern with predominantly severe damage to the thalamus and basal ganglia.
Additional Brain Imaging Methods for Hypoxic-Ischemic Injury
Magnetic Resonance Spectroscopy
MRIs can also be combined with magnetic resonance spectroscopy (MRS). MRS can help medical practitioners understand not just the impact of hypoxia/ischemia on brain structure, but also on brain cells’ metabolism.
Diagnosing HIE Using Ultrasonography (Ultrasounds)
Cranial ultrasonography (ultrasound) has the benefit of being available at the baby’s bedside. However, it has a low sensitivity for detecting the anomalies from hypoxic-ischemic encephalopathy (HIE).
Ultrasound has high sensitivity to show:
- Hemorrhages
- Ventricle size
- Severe parasagittal white matter damage
- Prominent cystic lesions
Ultrasonography does not show the outer portion of the cerebral cortex or milder white matter abnormalities very well.
Ultrasonography can be used to detect cerebral edema within about 24 hours after the hypoxic-ischemic insult. Findings include a global increase of echogenicity, or a brighter appearance on the ultrasound. Obliteration of spaces that contain cerebral-spinal fluid may be evident. After a few days, necrosis may show up as areas of echogenicity.


About ABC Law Centers: Birth Injury Lawyers
Birth injury is a difficult area of law to pursue due to the complex nature of medical records and imaging. The award-winning attorneys at ABC Law Centers: Birth Injury Lawyers have decades of experience with brain injury, cerebral palsy, and hypoxic-ischemic encephalopathy (HIE) cases.
We handle cases throughout the U.S. and have secured numerous multi-million dollar verdicts and settlements for our clients. Our team is here for you and ready to answer questions 24/7.



Featured Videos
Posterior Position
Hypoxic-Ischemic Encephalopathy (HIE)

Featured Testimonial
What Our
Clients Say…
After the traumatic birth of my son, I was left confused, afraid, and seeking answers. We needed someone we could trust and depend on. ABC Law Centers: Birth Injury Lawyers was just that.
- Michael
Helpful resources
- Hintz, Susan R., et al. “Neuroimaging and neurodevelopmental outcome in extremely preterm infants.” Pediatrics 135.1 (2015): e32-e42.
- Barnette AR, Horbar JD, Soll RF, et al. Neuroimaging in the evaluation of neonatal encephalopathy. Pediatrics 2014; 133:e1508.
- Executive summary: Neonatal encephalopathy and neurologic outcome, second edition. Report of the American College of Obstetricians and
- Gynecologists’ Task Force on Neonatal Encephalopathy. Obstet Gynecol 2014; 123:896.
- Wu YW, Backstrand KH, Zhao S, et al. Declining diagnosis of birth asphyxia in California: 1991-2000. Pediatrics 2004; 114:1584.
- Graham EM, Ruis KA, Hartman AL, et al. A systematic review of the role of intrapartum hypoxia-ischemia in the causation of neonatal encephalopathy. Am J Obstet Gynecol 2008; 199:587.
- Thornberg E, Thiringer K, Odeback A, Milsom I. Birth asphyxia: incidence, clinical course and outcome in a Swedish population. Acta Paediatr 1995; 84:927.
- Lee AC, Kozuki N, Blencowe H, et al. Intrapartum-related neonatal encephalopathy incidence and impairment at regional and global levels for 2010 with trends from 1990. Pediatr Res 2013; 74 Suppl 1:50.
- Sarnat HB, Sarnat MS. Neonatal encephalopathy following fetal distress. A clinical and electroencephalographic study. Arch Neurol 1976; 33:696.
- Ferriero DM. Neonatal brain injury. N Engl J Med 2004; 351:1985.
- Dammann O, Ferriero D, Gressens P. Neonatal encephalopathy or hypoxic-ischemic encephalopathy? Appropriate terminology matters. Pediatr Res 2011; 70:1.
- Executive summary: Neonatal encephalopathy and neurologic outcome, second edition. Report of the American College of Obstetricians and
- Gynecologists’ Task Force on Neonatal Encephalopathy. Obstet Gynecol 2014; 123:896.