Cephalopelvic Disproportion (CPD) Injuries
What is cephalopelvic disporportion (CPD)?
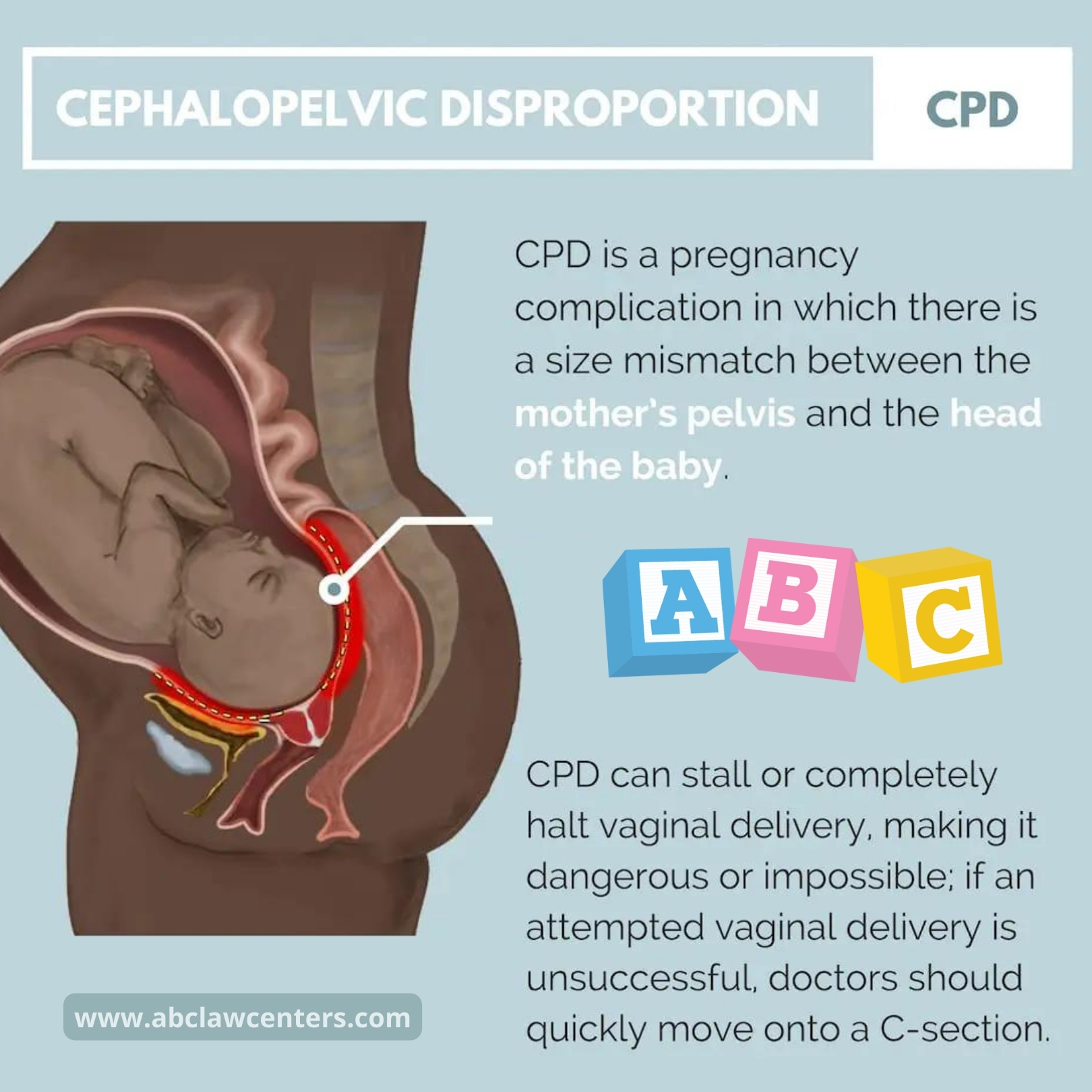
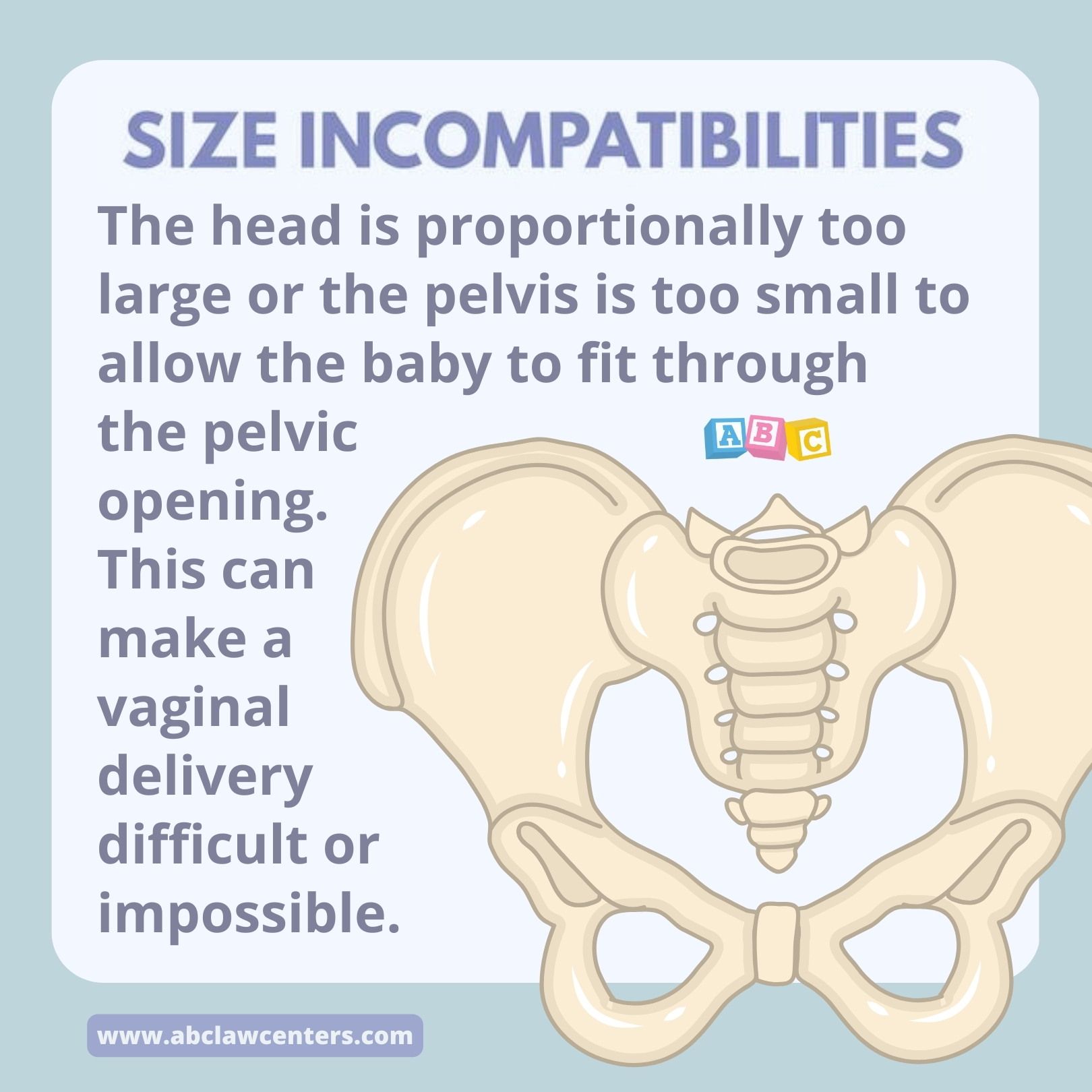
Cephalopelvic disproportion (CPD) is a pregnancy complication in which there is a size mismatch between the mother’s pelvis and the fetus’ head. The baby’s head is proportionally too large or the mother’s pelvis is too small to easily allow the baby to fit through the pelvic opening. This can make vaginal delivery dangerous or impossible.
If an attempted vaginal delivery is unsuccessful, doctors should quickly move onto a C-section. If they fail to do this, prolonged/obstructed labor from CPD may result in birth injuries such as hypoxic-ischemic encephalopathy (HIE) and cerebral palsy (CP).
Risk factors for cephalopelvic disproportion
Some women are more likely to have a pregnancy with cephalopelvic disproportion than others. Risk factors include:
- Infertility treatment
- Maternal obesity
- Previous cesarean delivery
- Polyhydramnios (1)
- Gestational diabetes
- Postmaturity or gestational age over 41 weeks
- Multiparity (mother has previously been pregnant) (2)
- Age 35 or over (advanced maternal age)
- Short stature (3)
- Transverse diagonal measurement < 9.5 cm (a measurement of the mother’s pelvis) (4)
- The mother has a history of childhood calcium deficiency or rickets (5)
- A variety of problems with the pelvis or birth canal
Causes of cephalopelvic disproportion
Cephalopelvic disproportion may be of maternal or fetal origin. In some cases the mother’s pelvis is unusually small; in others, the fetus’ head is unusually large. A combination of these two issues is also possible. Some causes of CPD include the following (6):
- Contracted pelvis: This occurs when a woman’s pelvis is smaller than normal in any important pelvic measurement (diameter).
- Pelvic exostoses: These are bony growths on the pelvis.
- Spondylolisthesis: This is a condition in which a bone in the spine slips out of its proper position onto the bone below it.
- Large sized baby: This can be caused by gestational diabetes and other conditions that cause a baby to be macrosomic (weight is > 4000 or 4500 grams) or large for gestational age (LGA). Post-term pregnancies and hydrocephalus (fluid in the baby’s brain that leads to swelling) may also cause cephalopelvic disproportion.
It is important to note that abnormal fetal presentations (i.e. when the baby is not in the typical position for safe, head-first delivery) can also make it difficult for a baby’s head to fit through the mother’s pelvis. Some consider this to be a form of cephalopelvic disproportion. However, it is distinct from what may be referred to as “true cephalopelvic disproportion,” in which the baby’s head is too large to easily fit through the pelvis, regardless of position (7).
Terminology may vary, but it is critically important that medical professionals examine the mother and fetus extensively enough to understand not only that there is something preventing the fetal head from making its way through the birth canal, but also exactly what the problem is. An appropriate intervention for an abnormal fetal presentation may do more harm than good in a case of true cephalopelvic disproportion. For example, forceps may be used in breech presentation or face presentation (8). This will not help a case of true CPD; if doctors fail to realize that forceps use is ineffective and continue attempting to deliver the baby that way, there may be birth injuries from excessive pressure/pulling.
Tell us your story.
A birth injury diagnosis for your child is difficult. If cephalopelvic disproportion was mismanaged during your pregnancy, our attorneys may be able to help. At ABC Law Centers: Birth Injury Lawyers, we focus exclusively on birth injury law & work with families just like yours.
Signs and symptoms of cephalopelvic disproportion (CPD)
The presence of certain conditions during labor and delivery indicate that there may be a case of cephalopelvic disproportion. If the fetus maintains a high station, even after a significant amount of contractions, this indicates that fetal descent through the birth canal may be difficult. Although it is not the only potential explanation, CPD should be evaluated as a possible cause of failure to descend.
Prolonged and arrested labor can result in oxygen deprivation, so medical professionals should also watch for signs of fetal distress.
Diagnosing cephalopelvic disproportion (CPD)
Listed below are several methods employed by physicians to try and assess the size of the pelvis and baby, which can help to diagnose CPD:
- Pelvimetry by MRI: This is used to assess the dimensions of the pelvis, determine the baby’s position, and examine the soft tissues of the mother and baby.
- Clinical pelvimetry: This is a process used to assess the size of the birth canal using the hands and/or with a pelvimeter.
- Ultrasound: The baby’s head and body size are measured during a routine ultrasound examination. Measurements are compared against standardized growth charts to determine the relative risk of CPD by the time of delivery.
- X-ray or CT pelvimetry: This is a radiographic examination used to determine the dimensions of the mother’s pelvis and the diameter of the baby’s head. The value of x-ray pelvimetry needs to be weighed against the risk of radiation exposure.
True CPD cannot always be clearly diagnosed before the beginning of labor. If medical professionals believe they may be dealing with a case of CPD but aren’t entirely sure, they may still attempt a vaginal delivery. However, they should be prepared to quickly move on to an emergency C-section or other interventions (see “Treatment for cephalopelvic disproportion”) if labor stops or the infant fails to follow the expected rate of descent. If true CPD is diagnosed prior to labor, a C-section may be scheduled in advance.
Treatment for cephalopelvic disproportion
Treatment for cephalopelvic disproportion (CPD) varies based on severity and when it is diagnosed. If it is severe and diagnosed early, a planned C-section is indicated. In other cases, CPD may be treated with a symphysiotomy (the surgical division of pubic cartilage) or an emergency C-section after a trial of labor. When CPD is present, continued attempts to deliver the baby vaginally can cause undue trauma and permanent injury to the baby.
Cephalopelvic disproportion and birth injuries
Physicians faced with cephalopelvic disproportion (CPD) must be very skilled in treating this potentially dangerous condition. Some complications that can occur when CPD is present can include:
- Overdose of Pitocin (synthetic oxytocin): One of the major problems with CPD is that physicians may react by administering Pitocin in an effort to speed up delivery. Too much of this drug may cause excessive and traumatic contractions, which can harm the baby.
- Prolonged Labor: Many physicians allow labor to progress for far too long. Labor is a trying time for the baby, and if it is prolonged, oxygen-deprivation injuries may occur. These injuries can lead to hypoxic-ischemic encephalopathy, cerebral palsy, and developmental delays. Furthermore, the trauma from continued labor may result in serious intracranial hemorrhages (brain bleeds).
- Shoulder Dystocia: When CPD is present, the baby is more likely to have shoulder dystocia injuries, including Erb’s Palsy or Klumpke’s palsy.
- Umbilical Cord Compression: When there is decreased room in the uterus, either because of a large baby or a small maternal pelvis, oxygen deprivation may occur due to a trapped umbilical cord.
When risk factors for CPD are present, it is essential that the physician monitor the mother and baby very closely and be prepared for a C-section delivery. In certain situations, an early delivery may even be necessary.
When should I call an attorney?
It is negligence when a mother and baby are not properly assessed and monitored. Failure to act skillfully and, if necessary, quickly, also constitutes negligence. If this negligence leads to injury of the mother or baby, it is medical malpractice.
If your child became injured at birth due to cephalopelvic disproportion – attorneys at ABC Law Centers: Birth Injury Lawyers (Reiter & Walsh, P.C.) can help. We’ve been working exclusively on birth injury law since 1997, which means that we have the knowledge and professional experience to determine whether there was an error or negligence, and to help you obtain the monetary compensation your child deserves. Contact us by calling (248)-593-5100 or filling out our contact form.


Legal help for cephalopelvic disproportion (CPD) injuries
If not handled appropriately, cephalopelvic disproportion (CPD) puts a baby at risk for numerous birth injuries. Physicians must recognize risk factors for CPD and follow standards of care to prevent the baby from being injured.
If your child was diagnosed with a birth injury due to CPD, please contact the attorneys at ABC Law Centers: Birth Injury Lawyers. We have helped children throughout the country obtain compensation for lifelong treatment, therapy, and a secure future, and we give personal attention to each child and family we represent. Our award-winning birth injury firm has numerous multi-million dollar verdicts and settlements that attest to our success, and you pay nothing unless we win your case.



Featured Videos
Posterior Position
Hypoxic-Ischemic Encephalopathy (HIE)

Featured Testimonial
What Our
Clients Say…
After the traumatic birth of my son, I was left confused, afraid, and seeking answers. We needed someone we could trust and depend on. ABC Law Centers: Birth Injury Lawyers was just that.
- Michael
Helpful resources
- Tsvieli, O., Sergienko, R., & Sheiner, E. (2012). Risk factors and perinatal outcome of pregnancies complicated with cephalopelvic disproportion: a population-based study. Archives of gynecology and obstetrics, 285(4), 931-936.
- Diabetes During Pregnancy: Symptoms, Risks and Treatment. (2017, February 22). Retrieved September 11, 2018, from http://americanpregnancy.org/pregnancy-complications/diabetes-during-pregnancy/
- Tsu, V. D. (1992). Maternal height and age: risk factors for cephalopelvic disproportion in Zimbabwe. International Journal of Epidemiology, 21(5), 941-946.
- Liselele, H. B., Boulvain, M., Tshibangu, K. C., & Meuris, S. (2000). Maternal height and external pelvimetry to predict cephalopelvic disproportion in nulliparous African women: a cohort study. BJOG: An International Journal of Obstetrics & Gynaecology, 107(8), 947-952.
- Brabin, L., Verhoeff, F., & Brabin, B. (2002). Maternal height, birthweight and cephalo pelvic disproportion in urban Nigeria and rural Malawi. Acta obstetricia et gynecologica Scandinavica, 81(6), 502-507.
- Maharaj, D. (2010). Assessing cephalopelvic disproportion: back to the basics. Obstetrical & gynecological survey, 65(6), 387-395.
- (n.d.). Retrieved September 11, 2018, from https://www.uptodate.com/contents/normal-and-abnormal-labor-progression?search=cephalopelvic disproportion§ionRank=1&usage_type=default&anchor=H102400915&source=machineLearning&selectedTitle=1~25&display_rank=1#H102400915
- Types of Forceps Deliveries. (n.d.). Retrieved September 11, 2018, from https://www.healthline.com/health/pregnancy/forceps-assisted-delivery#bottom-line